Erika shared her story in June of 2024.
There are times when I have to ugly-cry to my parents. You can’t go six years with chemo, radiation, surgery and physically depleting side effects and not need to cry. A lot of people don’t realize that I hurt a lot, most of the time. The side effects are constant. But I am really grateful to be alive. I don’t think there’s anybody who could possibly want to live as much as I do. I want to raise my six-year-old son, and I want to see my daughter, who is 21, flourish as an adult.
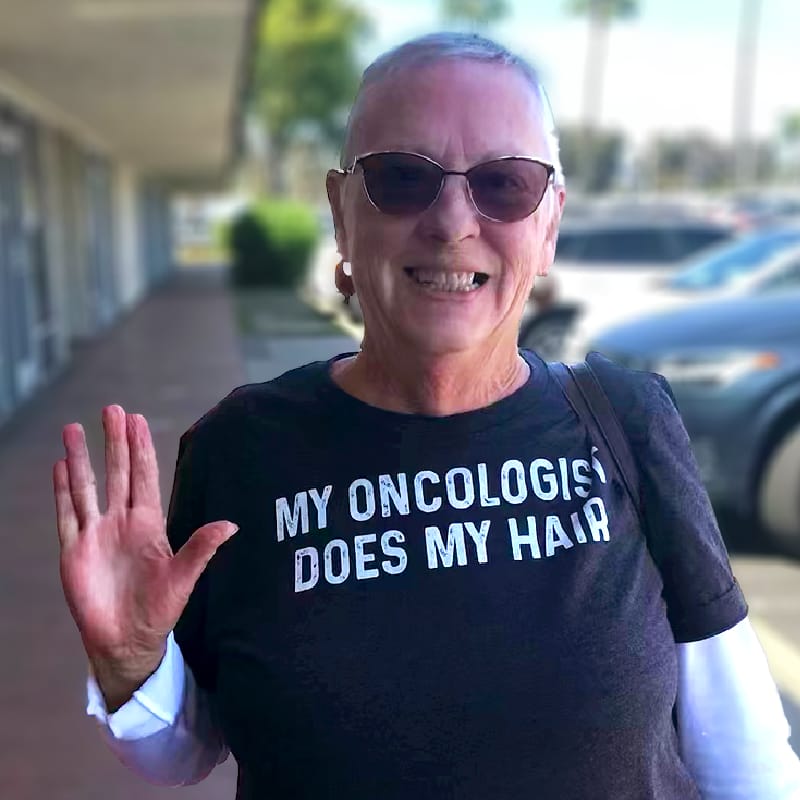
I was diagnosed with stage 4 breast cancer in February 2018 while eight-and-a-half months pregnant with my second child. Four days after diagnosis, labor was induced so that I could quickly begin treatment. I started chemo just two weeks after giving birth. I then moved back to Arkansas from New Mexico, in my fifth year of teaching at New Mexico State University, to have the support of my parents as I endured debilitating treatments and a mastectomy.
Since then my health has stabilized, and my scans have been clear for the last three years – after having large tumors on my liver, in my bones, in my breast, my lymph nodes and tailbone – but there’s still cancer cells, of course. Stage four is always there. I am never free entirely. And, anytime I have spoken to my oncologist about stopping treatment, they are adamant that that’s not a good idea. My oncologist says I need to stay on chemo as long as I can tolerate it, but the stability and clear scans give me some relief.
With this additional time – beyond enjoying reading, cooking, spending time with friends and family, and teaching social work – I’ve made a list of places I’d like to try and go with both my kids while my health is stable. We just visited Japan for the first time. We stumbled on a Buddhist Japanese wedding, and they let us watch. We went to see a big robot and a J-pop concert where people from age three to 80 were all doing the dance moves. It was a really special trip.
The relief from my clear scans, however, puts me in a weird in-between existence, between feeling almost normal and getting to continue a career I love full-time (despite ongoing chemo treatments every four weeks), and the other reality that my life is going to be shorter than I once anticipated.

Erika, Daughter siena, and Mom
Of course I’ve done all the legal stuff to prepare for the inevitable – who will make a decision if I lose consciousness, at what point I no longer want my life extended, what will happen with my assets and my kids – and had explicit conversations with my family. Now that I’ve had a little bit more stability with my health, the conversations are easier, more in the abstract. I’ve also had hard conversations about my more personal preferences. I made a list for my mom of the songs that she used to sing to me when I was little and asked her to sing those songs to me if I lost consciousness and I was dying for days, which is what I want to avoid. But if that happens to be the case (you can’t control everything), that’s one thing that’s important to me. Between that conversation and conversations about my children, those were the hard ones. None of it is ideal. But I do believe in having hard conversations. That’s what social workers do.
I’m doing everything I can to live well for as long as possible and make the most of the remainder of my time. But what I have learned in the hardest and most painful moments, when my tumors were large and my treatment intense, is that I want the ability to avoid a protracted and agonizing death.
Some people in hospice have peaceful deaths that just work out. I don’t want to discount hospice as a wonderful service, and I’d want to be on hospice no matter what. But that’s not always how it happens. Especially with cancer, the pain can be unpredictable and difficult to treat. Knowing that that’s what’s likely going to happen and that my mom and dad and my children are going to watch me in pain and vicariously experience that pain is gut-wrenching.
Medical aid in dying isn’t a political issue. I feel like we all want the control and peace of mind to be able to say goodbye to our loved ones and gently pass away. I would want to know that I’ve exhausted all of my options for treatment, that I’ve done as much as I can, that my health is to a point where it’s not going to turn around, that we know that this is going to end in my death no matter what. And ultimately, that I get to decide that my suffering is as much as I can shoulder, and I’m able to talk to my kids and my parents and my friends, and tell them the things I need to tell them.
People should be able to cultivate the end that they want. It is the culmination of their life.
Given my background in ethics and geriatric social work, and the fact that I was a supporter of medical aid in dying long before I got sick, I want to use the extra time I have to advocate for this option.
I think Arkansans are curious about medical aid in dying, especially with the residency requirements being dropped in Oregon and Vermont. This past year I’ve been asked by multiple Arkansas social workers to provide presentations about the topic. It’s an important conversation that’s happening and will continue, whether it’s authorized in Arkansas or not. Hospice social workers here have told me that people ask about the option often. As social workers, there is a professional duty to let people know where they can go for the healthcare options they seek.
My entire family is in support of me going wherever I would need to go to access medical aid in dying when the time comes. I want to be at home here in Arkansas, and ideally Arkansas allows for medical aid in dying by the time I need this option, but that feels like a far-fetched dream.
The next-best thing is Massachusetts passing legislation. That is where my brother lives and where my son would go to live if I were to die. The idea is that once I see my decline start happening, to go up there, still be a mother to my son as much as I can, and facilitate a transition for him to be with my brother and sister-in-law. That’s the hope. And then if I needed to use medical aid in dying, I’d be able to use it in Massachusetts. I could feel at home in Massachusetts in some sense.
But if Massachusetts doesn’t make medical aid in dying available, I’ll likely have to go to Oregon or Vermont. The idea of spending my last days dying somewhere unfamiliar is devastating.
I don’t think people consider how excruciating travel is when you’re unwell. When I was really sick, flying was very painful. I was traveling to MD Anderson cancer research hospital in Texas regularly, and it always hurt just to sit on the flight. Traveling at the end of life just isn’t always feasible. Cancer is sometimes a sudden and fast decline. I can plan to head to a state where I can use medical aid in dying, but in all reality I could be too ill to go because I, just like anyone else, want to live my life at home among the people I love and around familiar surroundings for as long as I can.
Mail contributions directly to:
Compassion & Choices Gift Processing Center
PO Box 485
Etna, NH 03750
Compassion & Choices is a 501 C3 organization. Federal tax number: 84-1328829